
This week's COVID-19 update with Dr. Bishop is jam-packed with information on breakthrough cases, the effectiveness of vaccines, fertility concerns, adverse reactions, and more. Watch the full video update below and read on for a complete recap.
Science Behind Breakthrough Cases
Why is it that we are having so many breakthrough cases of COVID, even if the symptoms are mild? What's the reasoning behind these breakthrough cases of COVID with people who have been vaccinated?
I don't have a solid answer for you. There could be a few things going on. When you get infected with a respiratory or a GI virus, one of the primary methods the body uses to protect you against that is a type of antibody called an IgA antibody, okay?
IgA antibodies are a type of antibody that's actually secreted out onto the surfaces of the mucosa in the body. So like the cheeks, the respiratory tract, the gut lining, all those areas secrete IgA.
And that is an antibody that's created more easily by natural infections, or by infections that happen via the oral or the nasal route. So when you get infected with a cold virus, for example, you're going to get antibodies to that virus that are both of the IgA class, and the IgG class, and the IgM class, but those surface antibodies really only get created when a viral infection happens from that entry point.
When you have a vaccine it's a little bit different. When you use an injectable vaccine, you generally get a very strong IgG response. That's a blood antibody. That is going to be a much higher level. You're going to get very minimal IgA antibody creation because you're not mimicking the natural infection route. You're injecting the antigen into the body, into the bloodstream.
You're not giving the antigen orally, or nasally, or anything like that. This is part of the reason that there have been these oral and nasal vaccines in the past. Polio used to be an oral vaccine. There was an attempt to have a flu vaccine that was a nasal spray for a while, and some of these others, because they do create a better IgA response than the injectable vaccines do.
So that being said, those IgA responses are probably a little bit better at preventing the virus from gaining entry into the body, but once the virus does get in, even though it may get in and set up a minor infection, the blood antibodies do come to the rescue at that point.
And that's why even though you're seeing breakthrough cases of COVID, the disease tends to be very mild, or very minor if you have symptoms at all because those blood antibodies do come in once the virus gets into the tissues and helps mitigate the course of the infection.
That's my sort of guess as to why we're seeing some breakthrough cases, because whatever IgA response you're getting from the vaccine probably is not lasting very long, and you're getting some natural waning of the IgG response, too, after a few months or so...
Booster Shots
Which brings us to the next question is: do I think we're going to have to have booster shots?
And I don't know yet. I think the problem we're going to find with boosters is that it may pump up that IgA response and reduce that transmission risk for a short period of time, but then you're kind of in a cycle where every six months you're needing boosters in order to keep the transmission risk low.
It seems that we're getting toward a year now on the vaccine testing that it seems to prevent hospitalization and death. All the vaccines seem to do an excellent job of this. Pfizer and Moderna especially do an excellent job of preventing hospitalization and death, even over the longer course. And that's really the more important outcome in my mind from the vaccinations is keeping people from dying and keeping them out of the hospital.
It really comes down to the booster question is about whether we're going to reduce transmission risk. And I'm not sure at that point if they're really going to want to be aggressive about pursuing boosters if it's just about reducing transmission, because what we're even seeing now is that this Delta variant is being transmitted at almost the same rate whether you're vaccinated or not, according to the CDC.
So I'm not sure where we're going to settle out on that issue over the next few months here, but it will be interesting to see what happens with that.
COVID Vaccine and Fertility
One other topic I want to touch on because it keeps coming up, and I keep seeing this in various places on social media and other places, our doctors keep getting calls and messages about this, too, which is this concern about the COVID vaccine and fertility.
There's a couple of things going on here. First, I've seen lots of strange things on social media about, oh, if you get the COVID vaccine you're not going to be able to have children. You're going to have fertility issues. There's no evidence for that.
A lot of this started from — this is kind of maybe going to be a little bit crazy — but an Amazon series, there's a whole WebMD article about this, an Amazon series called "Utopia." And the premise of the story was that the government, or whoever, releases a virus and then they give a vaccine. And the whole idea is to try to control the population. It's a fictional show, but it kind of took hold and became sort of this nidus for people getting this idea in their minds that the COVID vaccine does this. And then there was a few sort of off-the-cuff remarks by a couple of doctors about a particular protein issue.
The bottom line is that there's no strong evidence for this. There's no evidence at all that at this point that there are fertility issues with the COVID vaccine.
On the other side of that coin, we have very little data long-term showing safety in pregnant women or safety over the long-term. I don't want to overstate that either way, but I think the point is that just be very careful what you read online.
There's no evidence showing that the vaccines are harmful to fertility. There is no long-term data on the vaccines either. There are a few pregnant people in the original studies for the COVID vaccines and they had no problems, and that's great.
We don't have large-scale studies on pregnant women. There are lots of pregnant women who have taken the vaccine and have had no problems.
I suspect over the next couple of years, we're going to find that the vaccines probably are safe in pregnancy, in terms of they're probably not going to have any impact on fertility.
We don't know that yet, but we also have no evidence to say that you're going to have fertility problems, so if you hear people saying that, say, hey, that's not true. There's no evidence to suggest that. And I think it's irresponsible for people to sort of be spreading that information it's not accurate.
So that's the thing on that. So please just continue to be careful what you read online. It's a wild world out there so just be cautious, so, okay.
Pfizer and J&J Breakthroughs vs. Moderna
"I have heard that those with Pfizer and J&J have had breakthroughs, but those with the Moderna have not. Is there data to actually support that?"
I have not seen data showing that there are any differences or issues with the Pfizer or Moderna vaccine.
It's widely known from the trial data that the J&J vaccines are not as effective as Pfizer and Moderna for transmission, for infection, for mortality risk, for high hospitalization risk, that it just doesn't work as well. And that's clear from the data from the published trials by J&J.
But I've not seen that there's been a big difference of breakthrough infections for Moderna. It seems to be happening to a little bit of both, but that's just my anecdotal experience. I haven't seen any data breaking that down by which vaccine people got. So perhaps we'll see that in the coming months.
Spleen Removal and Boosters
"Should a person without a spleen who received the J&J vaccine be looking to get a booster, or at least get antibody testing?"
I think that's an interesting question. I think that we've seen more of a call for looking into boosters for people who have problems with their immune systems, and people who have no spleen do certainly have trouble with antibody formation against certain types of things.
If you're concerned about that, I would talk with your doc, and it might be reasonable to get antibody testing to make sure you've got a sustained good response to the J&J vaccine. I do know that a city in California is going to start offering what they're calling supplemental vaccines with one of the mRNA vaccines for people who got J&J, I think with an eye toward people who have potentially compromised immune systems maybe taking advantage of that.
I'm not aware of anyone locally here offering boosters, or supplemental vaccines, for anyone regardless of whatever vaccine type you got first, but that's something you might want to be talking with your doc about to get on the radar to get the testing done just to see, so good question.
Vaccinations after COVID Infection
"What is the thought about getting the vaccine for those that have natural antibodies from a past infection?"
Yeah, good question. CDC, FDA, everyone, all the major guidance bodies continue to recommend that people who had COVID get a vaccine afterward. And I think that that is a totally reasonable thing.
We don't know how long the immunity from natural infection lasts. There's a lot of variables in there, depending probably on how sick you got initially and some other things.
That being said, I think if you had natural infection, it's not unreasonable to get yourself tested for antibodies, and see if you still have antibodies, and let that play into your decision about whether to get vaccinated or not. I think that's a reasonable course of action, especially, if you had a fairly significant illness with COVID.
If you were very minorly ill, like you just had a stuffy nose, or what have you, I would still consider getting vaccinated because your immune system response is probably not extremely strong because you didn't get very sick.
That sounds a little counterintuitive, so I think it depends a little bit on how ill you were when you got COVID, but a reasonable thing to do to get the antibodies checked. And if they are low, or are not there, then I would go ahead and get vaccinated for sure.
If you still have strong antibodies, then I think that's a conversation you could have with your physician about whether it still might be a good idea to get vaccinated, or if you want to wait a bit. I think that's up to you in that case.
That being said, the official recommendation is still to get vaccinated if you've had COVID before, so keep that also in the back of your mind.
Booster Trials?
"Are there any COVID-19 booster trials going on right now that you're aware of?"
The only one that I'm aware of currently, Pfizer released a small, small study. It had about 20-something patients in it. And that is the only trial that I am aware of currently. I think Pfizer is still recruiting for larger trials on that, but I haven't seen anything from Moderna just yet.
I do know that the Israeli government is going to start offering boosters to its elderly folks, 65 and up, so that's going to be sort of a natural experiment in the coming months and weeks, and we'll see what effect that has on their population in terms of transmission rates, etc.
So that will be interesting to see, but I think Pfizer is the only one that I'm aware of right now doing it. I bet Moderna is too. I just haven't seen the data on it to be honest, and it may just not have been released yet, so, good, good questions.
Case Numbers in Perspective
I know we're all very worried about the Delta variant, and I think rightly so because cases and hospitalizations are up, and that is concerning.
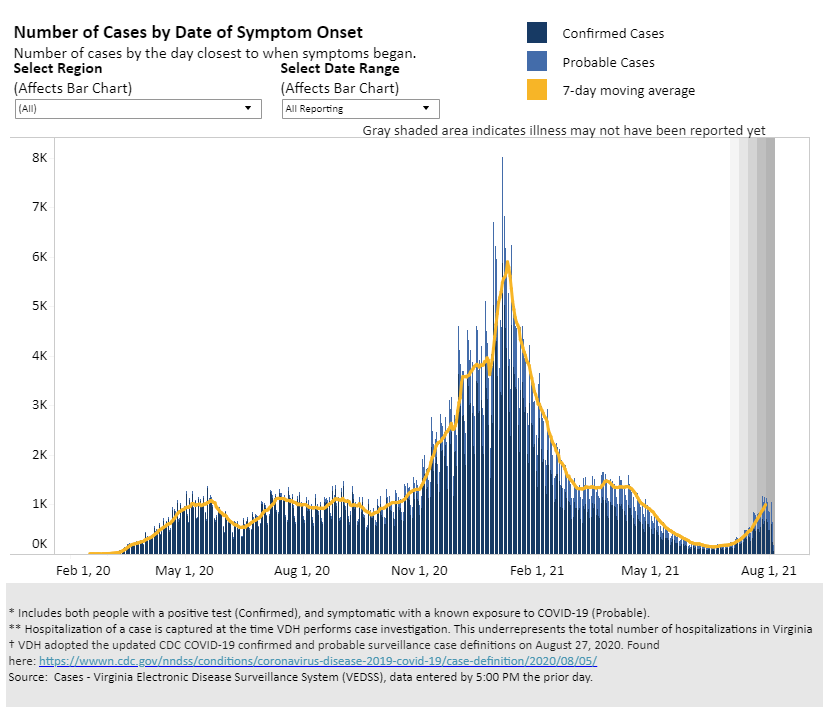
I think it's important, though, just for some perspective, to keep things a little bit in mind about where we really are with things. So I'm going to link the Virginia Department of Health case dashboard.
And what you should do when you get on there, I want you to go to the page where you're looking at cases, hospitalizations, and deaths and you'll see down there at the bottom where you can look at the graph in the chart, and see where things are.
And when you do that, I want you to change the reporting range to all available data. Because it gives you a little bit of a better perspective on what's going on versus just looking at the 90-day window, right?
Things are getting a little bit worse the last few weeks, but if you zoom out and look over the last six months, or since last year, what you're really seeing is a small blip.
It's a blip, but it is small compared to what we saw say over the holiday season last year at least currently. We'll keep watching, of course, and see how things go, but it's good just to keep things in perspective, okay. So just zoom out a little bit, and take a look at that information. And I think that might be helpful to some folks.
(Editor's Note: Here's the chart Dr. Bishop references.)
Different Boosters?
"Is a booster given today a different vaccine or just a third dose of the same?"
I believe what they are testing is a third dose of the same formula so nothing new.
Adverse Reactions
"We really need a comprehensive approach to diffuse the fear, honesty, and treatment for vaccine adverse reactions. We all know they're not 100%. Why not talk about what to do if you become sick? Why should anyone risk it if they'll become a ghosted statistic? Why aren't we talking about early treatment?"
Yeah, so two great questions. First thing, I think we do need to be honest and transparent about vaccine adverse reactions, and I think, for the most part, most physicians and others are trying to be as honest and transparent as they can about what we're seeing and what's being reported in the data.
There certainly are some adverse reactions. That being said, they are pretty rare overall. There are some cases of things like Bell's palsy, Guillain-Barré syndrome, anaphylaxis, things of that nature. All vaccines have side effects. The myocarditis, pericarditis that we're seeing in young adolescent men, in particular, is certainly real and it's definitely there.
The risks are not zero. The risks are low, however. And you do have to balance those risks of vaccination with the risks of getting the natural illness, right?
COVID, of course, can cause all of these things too. Myocarditis, blood clots, permanent lung damage, Guillain-Barré, all these things, ITP. All these things COVID can cause as well.
I think for the vast majority of people, adults say 30 and up, your risk of having an adverse outcome from a vaccine is pretty small. Almost vanishingly small.
You're much more likely to have a problem from natural COVID infection than from a vaccine, especially, if you're 30 and up. Definitely, if you're 40 and 50 and up.
The risks of getting natural COVID are far, far, far higher than having an adverse reaction from the vaccine the older you get. Definitely in the 30s Certainly in the 40s. Absolutely, without question in the 50s getting COVID is a much higher risk proposition than taking the vaccine.
As you get younger into the 20s and the teens, I think that discussion becomes a lot more nuanced, depending on the health status of the person. I think we do have to be transparent about that on both sides.
How VAERS Works
I think something that does concern me about the discussion around adverse events related to COVID vaccines is that people don't understand how the VAERS system works. This is the Vaccine Adverse Event Reporting System that the CDC and the FDA use to track adverse events from vaccines.
That system is an early report system. Any physician, or any other care provider who sees a potential adverse outcome from a vaccine, they report it there.
That doesn't mean necessarily that what they're seeing is certainly from the vaccine. It means that they have a patient who recently got a vaccine, and something happened to them.
Those things all get investigated and adjudicated. And when it's determined that either, yeah, that reaction was certainly from the vaccine, or, no, this is completely unrelated, that data gets updated.
And I think what's happening is we have people looking at the VAERS data, which is publicly available, which is great, and saying, oh, all these deaths are reported, or these X, Y, or Z things are reported from the vaccine.
That does not mean that those things happened because of the vaccine. It means those things happened around the time of the vaccine. If you give enough of any medical intervention to enough people, random things are going to happen to them. People die in car accidents, people die of heart attacks, people die of strokes, people die of old age, these things happen, right? And they may happen around the time you get vaccinated. That doesn't mean the vaccine caused it.
So while I think it's good, we need to be completely transparent about that data. I think people need to know that just because something is put into that VAERS database, it does not mean that that is from the vaccine. It just is an early warning system for doctors, especially, to report potential adverse outcomes, so that people can investigate them. So I think we just have to be a little bit careful with that.
Early COVID Treatments
In terms of early treatment, I continue to be a little bit befuddled why we are not talking about some of these things.
There's been a lot of additional data that has come out about ivermectin, in particular. We are using it here periodically for our patients when they are relatively sick as early treatment. There have been a number of meta-analyses done on ivermectin at this point, and the data seems fairly strong. Strong enough to use it because of the safety profile of ivermectin.
I think we do need to be talking about that more, but I think that that discussion is getting drowned out about all the drama related to vaccines, so, a lot going on there for sure.
Delta Variant Peak?
"The Delta variant in the UK peaked and plummeted. Would the scenario be expected here?"
I don't know. I hope so. I certainly hope that is the case. And we may find that. I think we're just going to have to wait and see.
We're going to keep getting waves of infection regardless of whatever the current variant of the month is until we do have enough people vaccinated and/or immune to it in whatever way. So we're going to keep seeing these waves.
Hopefully, they become lower and lower amplitude waves over time as more and more people get vaccinated, but I would expect, yes, that there to be sort of a wave, and it to die down.
And then we'll have probably another one in a couple of months. And we're going to, again, keep having these waves until the pandemic wears itself out essentially.
Delta Variant and Herd Immunity
"I saw a small article that suggested Delta variant may achieve herd immunity?"
Good question. I don't know. I think it's going to depend on a lot of factors. Regardless of whatever the variant is, we will eventually get to herd immunity one way or another. Either enough people will get vaccinated, or enough people will be vaccinated plus have natural infection, that herd immunity will be achieved one way or another. That is just the way that viruses work.
And it depends, the time course of those things, and how much suffering we have. Those are two sorts of different paths.
I think the more people who are at risk — again, the 30s and 40s, 50s and up — the more people get vaccinated, the better, and the less suffering we're going to have while we get to herd immunity.
We will get to herd immunity one way or the other. That is just the way that biology will play out.
Large Gatherings Right Now?
"Would you recommend against large gatherings at this time given Delta?"
I think it depends. I think, for most people, if you're vaccinated, if you are young and healthy and you are not worried about your personal risk, I think that it is fine to go ahead and continue business as normal.
The data is quite clear. The vaccines work in terms of reducing the risk for hospitalization and death. They're very, very, very effective. If you've been vaccinated, or you're young and healthy and not worried about your risk, I think it's okay to continue as normal.
If you have not been vaccinated yet and/or you're otherwise worried about your health in terms of your immune system, you have a lot of medical problems, I think you might want to be considering that a little bit over the next few weeks and whether you want to start being a little bit more vigilant about social distancing, washing your hands, things of that nature.
And I think, again, if you're someone who's at the point where you're worried about your health status in terms of whether you can be at a large gathering or not, I think that that should give you a little pause, and really strongly consider whether that means you ought to go ahead and just get vaccinated so that you can take that risk off the table. And I would recommend that very strongly for people.
Large Gatherings, Part II
"Having a college sendoff this weekend, everyone will be vaccinated with the exception of one person who had COVID last year. Would you ask this person not to come? There'll be about 25 people there, including grandparents."
That's a tough question. You guys will have to kind of make a tough choice on that. That being said, I think if that person had COVID last year, odds are they're not going to be a source of transmission for you in all likelihood.
If it were my family gathering, I would not exclude that person because of that. And I think they're probably perfectly safe to come, especially, if all the high-risk people are vaccinated, right?
That's the thing, the vaccine really, I think, we're going to have to shift our thinking a little bit on the vaccine in order to align ourselves with the science, which is the vaccine is about reducing your personal risk of a bad outcome with COVID. It's not really about the transmission issue.
The vaccines are very, very effective for preventing hospitalization and death from COVID for the receiver of the vaccine. Whether you've received the vaccine or not, you can still be a vector, especially for the Delta variant. So frankly, someone who's vaccinated may be asymptomatic and transmitting the virus, especially the Delta variant, because they got infected with it, but they have minimal to no symptoms.
So a vaccinated person could come to your event, and be spreading the virus and you wouldn't know. I think the more important thing is to make sure that everyone who's going to be at the event, that they've reduced their personal risk of doing poorly with the virus through getting vaccinated if that's something that you're worried about.
I would not exclude someone just because they might be a vector, or a transmitter, because frankly at this point that could be anyone, vaccinated or non-vaccinated, okay.
Common Thread for Breakthrough Infections?
"Has a common thread been found in those who had a breakthrough infection and died?"
Not that I'm aware of yet. I am confident that we will see data on this in the coming weeks. The only things that I have seen are they tend to be the people you would expect, right? People who have lots of medical problems to start with who perhaps either didn't respond well to the vaccine or they're just at such high-risk from doing poorly that they were going to do poorly even after vaccination because, of course, the vaccines aren't perfect, right? Nothing is.
There's still going to be a small percentage of people who don't do well despite being vaccinated. That's always going to be true. It's a very tiny number of people.
Just talking to colleagues in the area, the number there are, as far as I'm aware, few to none vaccinated individuals in ICUs in the local area.
The vast, vast, vast majority of them, essentially all of the people in ICUs in the local area here, are unvaccinated patients. Take that for as it is at face value.
Again, the biggest way to reduce your risk is to get vaccinated, especially if you have medical problems, or you're older.
Outdoors Still Safer?
"Does being outdoors still help for lowering risk or did it change with Delta?"
Yeah, it's still a lower risk. It still is a lower risk to be outdoors than indoors for Delta for sure.
Breakthroughs in the Elderly?
"Aren't the majority of breakthroughs who died in the very elderly?"
I believe that is true. It's not exclusively true, but I believe that is true, yes. And, again, it's people who you would expect not to respond as well to vaccination in general because they're older, their immune systems are not quite as active or responsive, so that perhaps they just didn't have as good of a response to the vaccine as we would hope, so certainly possible.
Topics:
{kind=link}